Some months ago I was asked by Paul Rosenfeld, who directs psychiatric training at Mount Sinai Hospital Morningside West, to give a lecture. This took place on January 18. There was a Q and A afterwards. The talk was recorded and the video is here – Relationship Based Medicine.
There will be two related talks, which will also feature in posts soon. Relationship Based Medicine was delivered to clinicians. The next is an open public lecture, which will take place in Lethbridge Alberta today – Thursday January 26, and is called Beware Doctors Bearing Gifts. The final one will be in a few weeks time to a mixed group of lawyers and doctors. There are some overlaps but each talk brings different issues into play.
As per the YouTube and Podcasts message, it would be good if people could subscribed to the YouTube channel – subscribe does not mean hand over money.
The slides and text of Relationship Based Medicine – the original title for which was Standardizing Psychiatry and its Clinicians (Slide 1) – are below.
{kind=link}
Slide 2: The date on this suicide note is October 2004. Concerned that FDA planned to put a Black Box Warning on antidepressants for minors APA state they believe ADs save lives.
Saying suicide note or as I will say later the Art of Medicine involves bringing good out of the Use of a Poison might make you think I’m anti-drugs or the medical model. I use medicines and ECT rather than any other form of treatment and believe in the medical model. But the art of using these treatments also means knowing when not to use them.
{kind=link}
Slide 3: APA should have said they believe Clinicians save lives. The magic should lie in you not in pills.
But the processes of standardization affecting all of health festoon antidepressants with numbers. These look like science but aren’t. You make or should make judgments and choices, which cannot be standardized. These do not look like science but are.
In addition, making judgments is a moral enterprise – simply using antidepressants is amoral.
{kind=link}
Slide 4: The crisis bothering APA began 15 years earlier with this paper, in which 3 clinicians claimed fluoxetine caused 6 people to become suicidal. The causal claim was based on analyzing the cases closely and followed traditional clinical approaches for determining causality. There were about 10 other groups reported similar findings.
{kind=link}
Slide 5 I contributed to this debate, outlining the cases of 2 men, challenged with an SSRI, then dechallenged and rechallenged. There was no other way to explain what happened except that fluoxetine had caused it.
{kind=link}
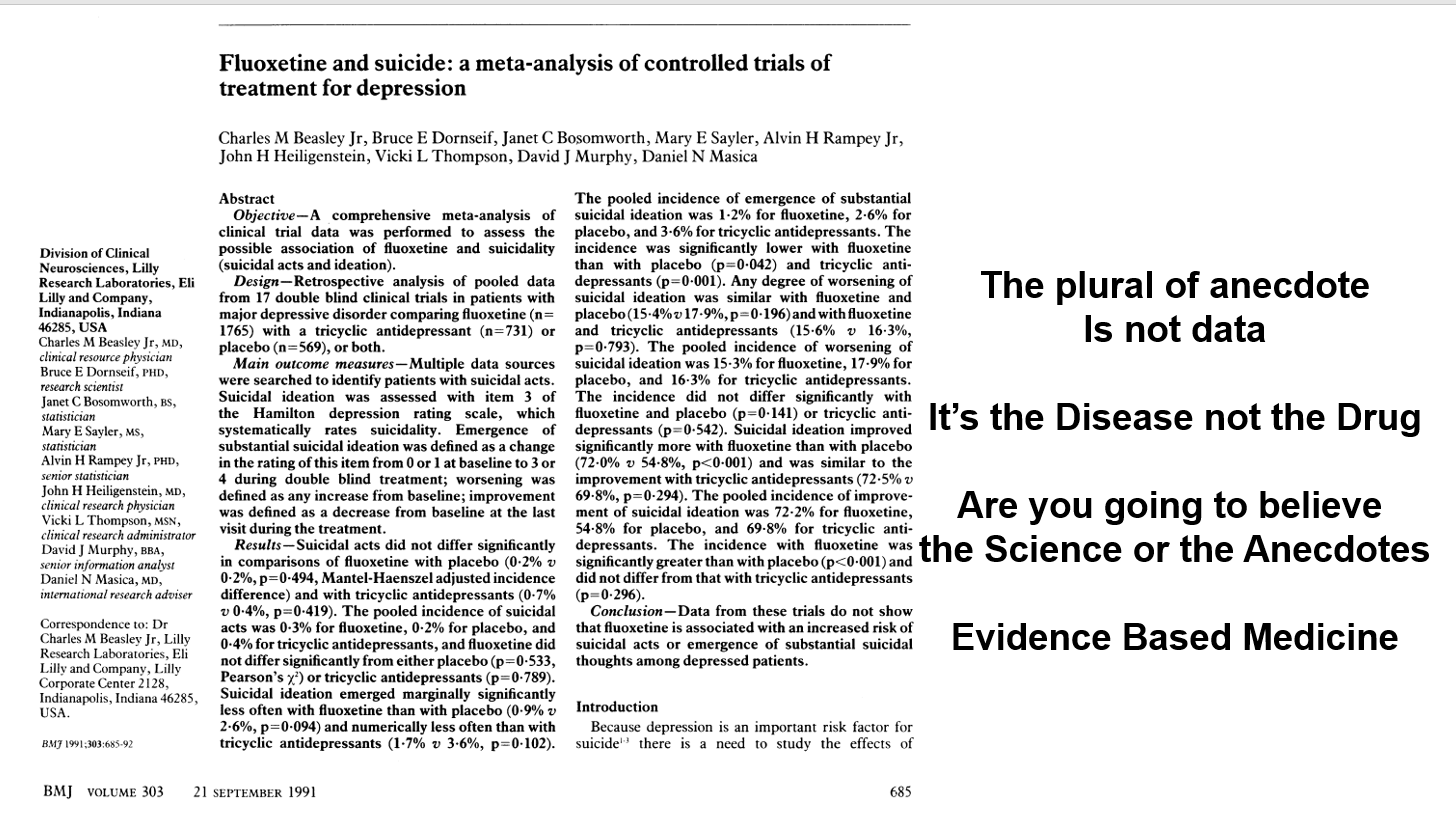
Slide 6 Almost the same week this Lilly article came out in the BMJ claiming an analysis of their clinical trials showed no evidence fluoxetine made people suicidal. The cases reported were sad but anecdotal and the plural of anecdotes is not data. Depression was the problem not fluoxetine. Clinical trials are the science of cause and effect.
This paper created Evidence Based Medicine and the question to doctors, the public, the media, politicians was – are you going to believe the science or the anecdotes?
In fact, the original phrase is the plural of anecdotes is data – otherwise Google wouldn’t work.
The idea the disease was responsible for suicide attempts and suicides in healthy volunteers or patients in trials with anxiety or OCD was hard to believe but some experts claimed just that.
Finally, what I hope to show you is the Teicher et al paper was Evident Based Medicine whereas Lilly’s Evidence Based Medicine is artefactual.
{kind=link}
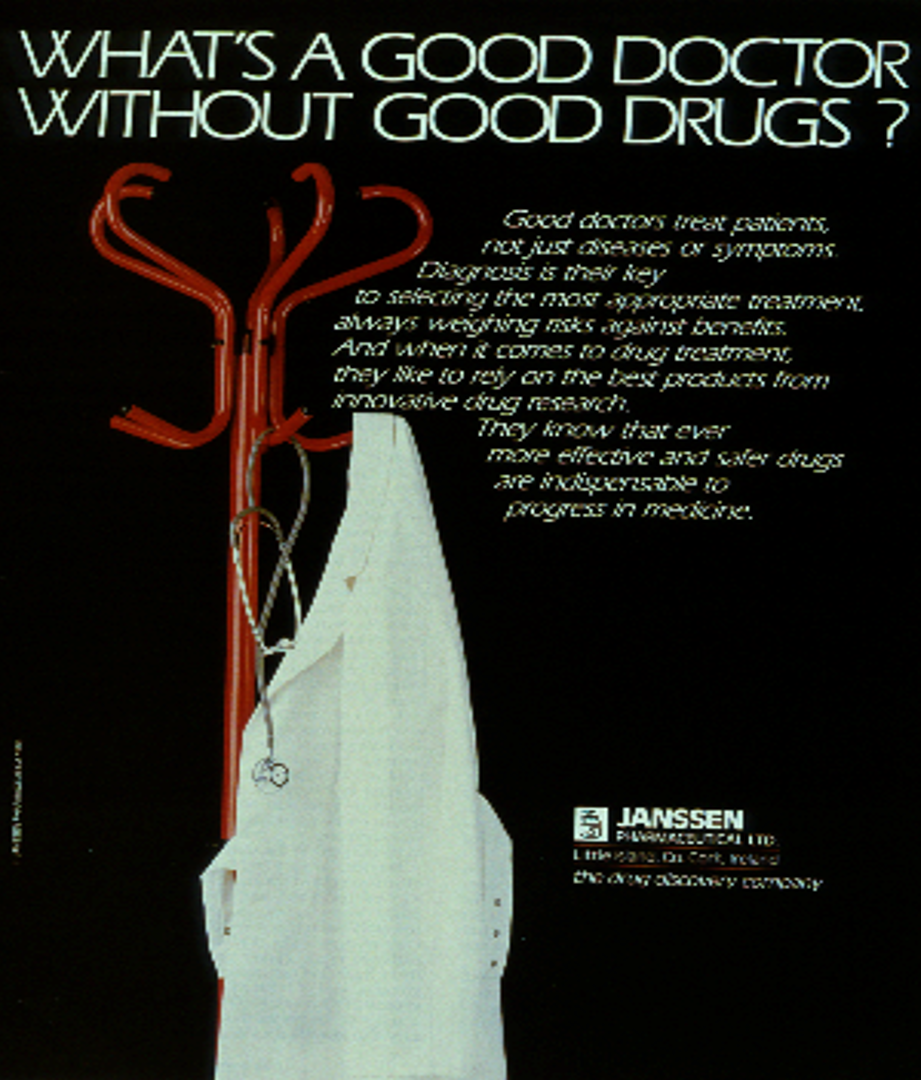
Slide 7: The Art and Science of Medicine are often contrasted. Those in the soft human sciences contrast their rich qualitative context with the experimental context, where hard scientists eliminate confounders with RCTs. This pre-Risperdal Janssen Advert assumes you will figure that paying heed to the soft side of things is a touch twentieth century.
My argument is the Science of Medicine lies in making hard judgement calls. A made by algorithms medicine may make your life easier but will doom Us. By Us I mean the chance of a community. Following the Artefact alienates you from Us.
{kind=link}
Slide 8: The origin of science story usually starts in 1660 when The Royal Society came into being. This established the ground rules of Science.
Science would deal with philosophy or theology. It would only deal with matters that could be Settled by Data. The focus since has been on the Data, but participants were called on to make judgement calls about the data in front of them. If you were Xtian, Hindu, Jew, Muslim, or Atheist, you left these badges at the door and had to explain what you saw without appealing to a Book or Authority.
You could run the experiment again, adapt the apparatus, check it out for tricks – what you couldn’t do was refuse to come to a Verdict about the data.
{kind=link}
Slide 9: This account of our history overlooks an equally important event 44 years earlier, when Walter Raleigh had his head chopped off – supposedly for being too close to those pesky Europeans. Raleigh was convicted on the basis of things said about him by people who did not come into court to be cross-examined.
Legal systems worldwide recognized the injustice of this and introduced Rules of Evidence. Hearsay could not be used as evidence. The only evidence that can be used in court is material that can be put in front of jurors who can see the people or material being examined and cross-examined. The process of forcing 12 people with very different biases to come to a Verdict about what is in front of them is the essence of science.
Verdicts and diagnoses are provisional – the view that best fits the current facts. If the facts change, we reserve the right to change our mind. This might appear to contrast with the objectivity of science, but scientific views are similarly provisional. Scientists attempt to overturn verdicts with new data.
If I gave fluoxetine to Paul 30 years ago and he came back suicidal. I could examine and cross-examine him, run lab tests and scans, raise the dose, stop the drug, add an antidote, check with colleagues has anyone else seen anything like this or can they explain it in any other way.
If Paul and I conclude fluoxetine has made him suicidal and report this to FDA, the first thing FDA does is to remove his name. No-one can now examine or cross-examine him and come to a scientific view about whether there is a link or not. His injury has been made Hearsay.
If you are later injured in the same way and see 1000s of reports of suicidality on SSRIs on FDA’s adverse event reporting system, you cannot bring this evidence into court because no-one can be brought into court. It’s Hearsay not evidence.
Company assays are all Hearsay – they should not be let into Court as evidence. Names count. Paul in this case is the data and accessing the data means accessing him.
If Paul and I report his case in a journal as a Case Report, with our names on it, either of us can be brought into Court. Case reports are the best evidence we currently have in clinical psychiatry – the only material that reaches standards of evidence.
{kind=link}
Slide 10: Here 20 years after he created the first RCT, is Tony Hill saying RCTs can be helpful for assessing one of the 100 things a drug does – and this might be useful for treatment purposes.
If RCTs evaluate only one of a 100 things a drug does, by definition they are not a good way to evaluate a drug. Hill was clear that clinical judgement should not be replaced by an algorithm.
All RCTs generate ignorance, but they can be useful provided we remember that some can also generate useful information – we can bring good out of this artefact.
{kind=link}
Slide 11: This 1960 placebo controlled RCT makes Hill’s point well – thalidomide has therapeutic efficacy as a sleeping pill but the trial shows nothing of the SSRI-like sexual dysfunction, suicidality, agitation, nausea and peripheral neuropathy thalidomide causes. Louis Lasagna was the person two years later responsible for incorporating RCTs in the 1962 Food and Drugs Act amendments.
{kind=link}
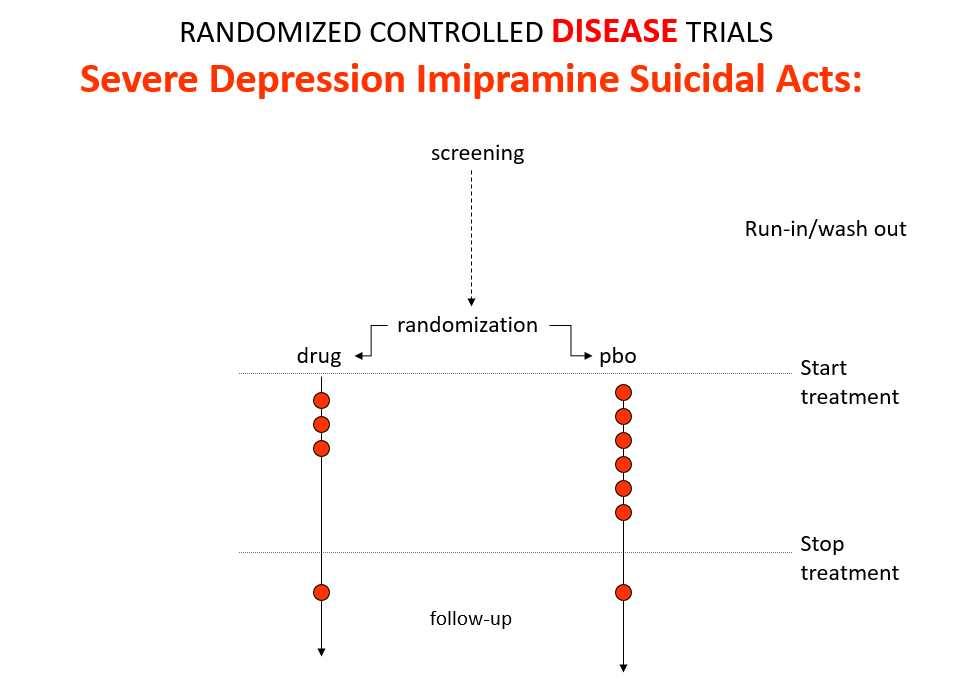
Slide 12: Some people say RCTs can demonstrate cause and effect in a way that other study designs can’t. Imipramine was the first antidepressant. It and other tricyclic antidepressants are stronger than SSRIs and SNRIs. They beat SSRIs in RCTs. They can treat melancholia – SSRIs can’t. Melancholia comes with a high risk of suicide.
Imipramine was launched in 1958. A year later at a meeting in England, Danish psychiatrists made it clear that while it was a wonderful treatment it made some people suicidal.
Let’s do a thought RCT of imipramine versus placebo in melancholia. Even though it can cause suicide, we would expect it to reduce the number of suicides in a trial like this because it treats the condition. This RCT would be great evidence antidepressants do not cause suicide.
{kind=link}
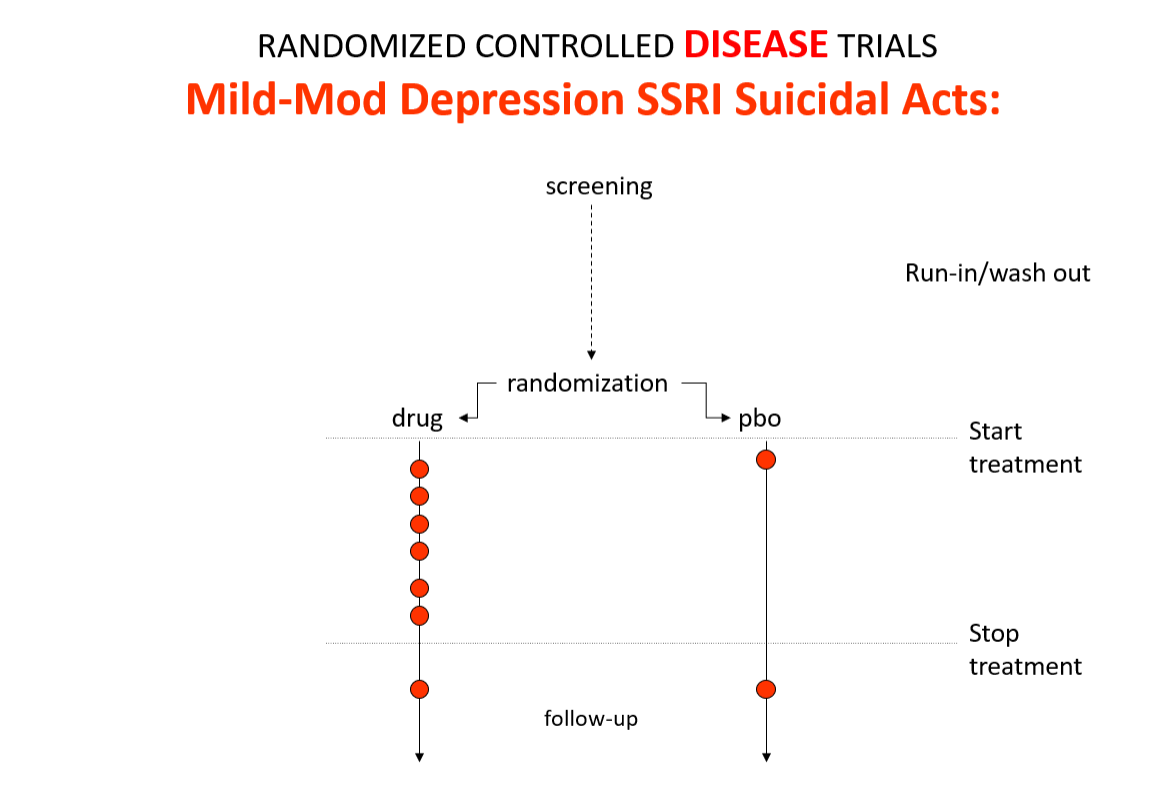
Slide 13: Here is the data on the trials in mild depression that brought the SSRIs and SNRIs on the market – you see a doubling of suicidal events compared to placebo. Companies resorted to all sorts of illegal maneuvers to hide this risk.
{kind=link}
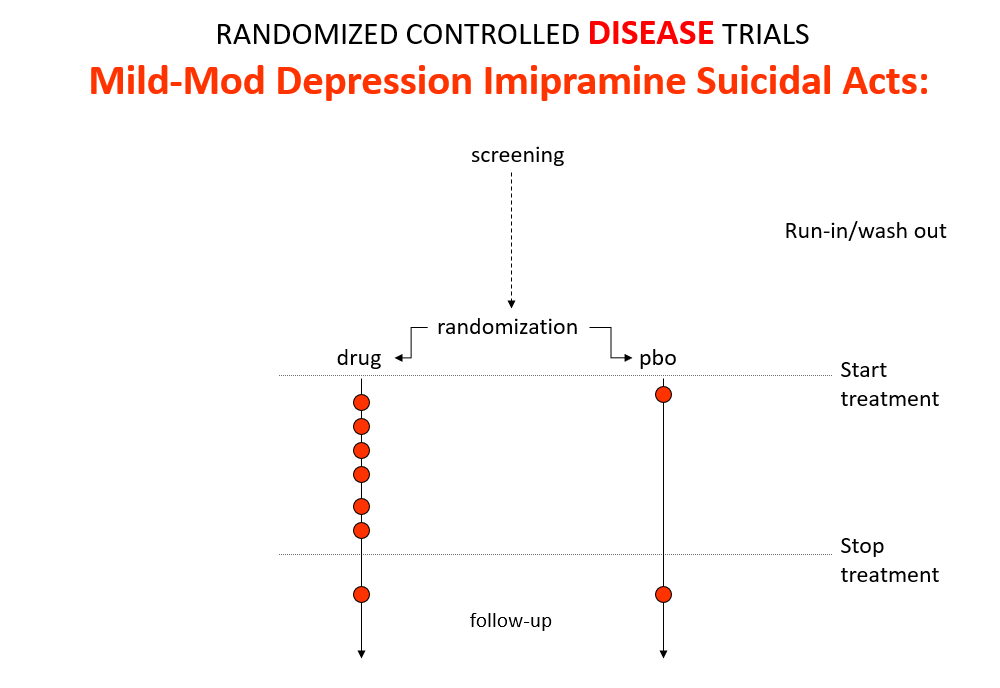
Slide 14: This is what the data for imipramine look like in the same mild depressions. Now it seems that it too causes suicides. So RCTs tell us nothing about cause and effect – they can give us diametrically opposite answers. This is because these aren’t drug trials. They are Treatment Trials and in any clinical Trial, the condition confounds the effects of the drugs – and these confounders hide drug effects.
People evaluating drugs in traditional clinical trials, before RCTs, knew this. People doing RCTs don’t. When a patient becomes suicidal in a trial you have to use your judgement to work out what is happened but in RCTs clinicians are not supposed to use their judgment.
This is not just the case for depression – it’s true in every clinical situation where drugs and conditions cause superficially similar effects – diabetes and glitazones both cause heart failure, osteoporosis and bisphosphonates both cause fractures
{kind=link}
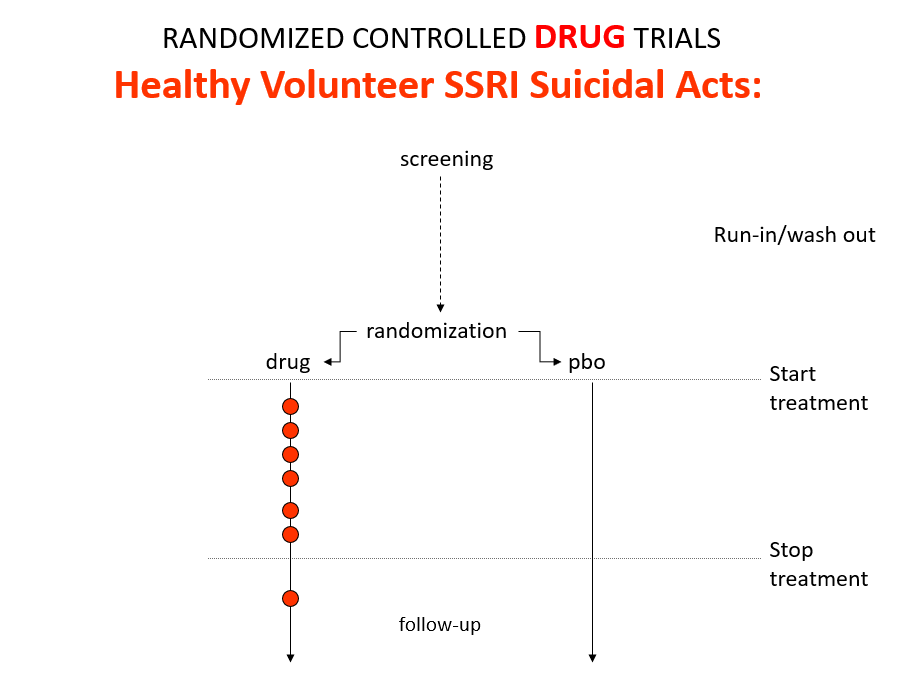
Slide 15: Here is what a drug trial looks like. Companies ran these studies in the 1980s and found that SSRIs make healthy volunteers suicidal, caused dependence and sexual dysfunction but we heard nothing about these problems when the drugs launched. These Drug Trials enabled companies to engineer their Treatment Trials to hide these problems.
{kind=link}
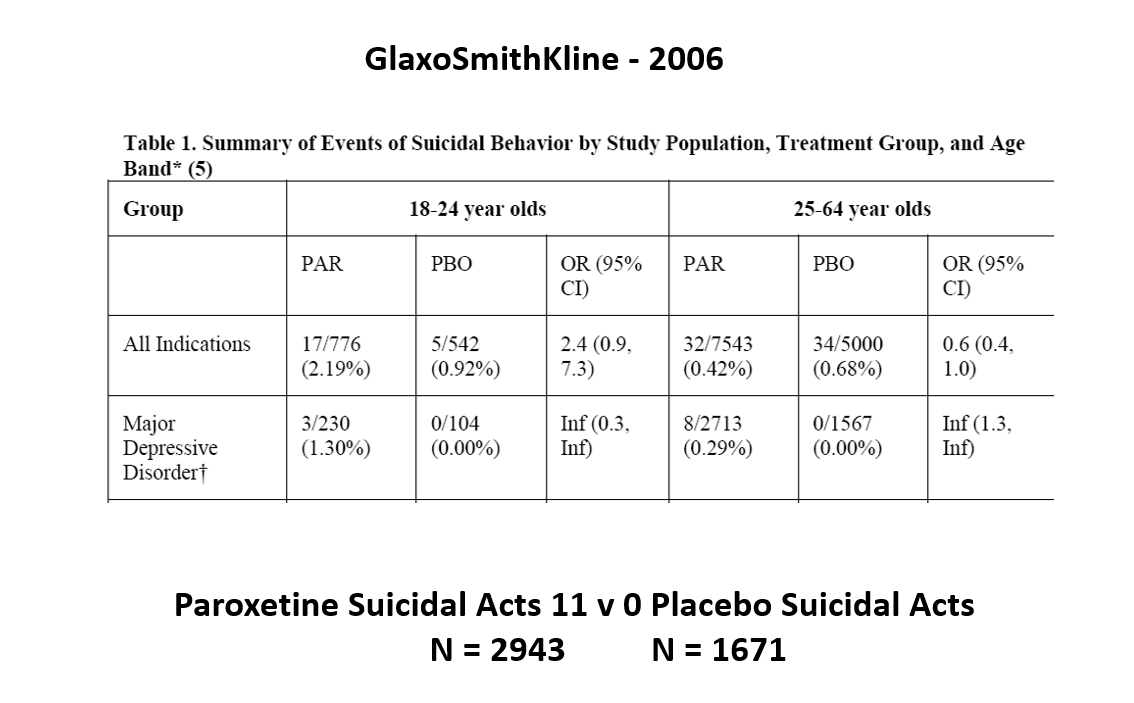
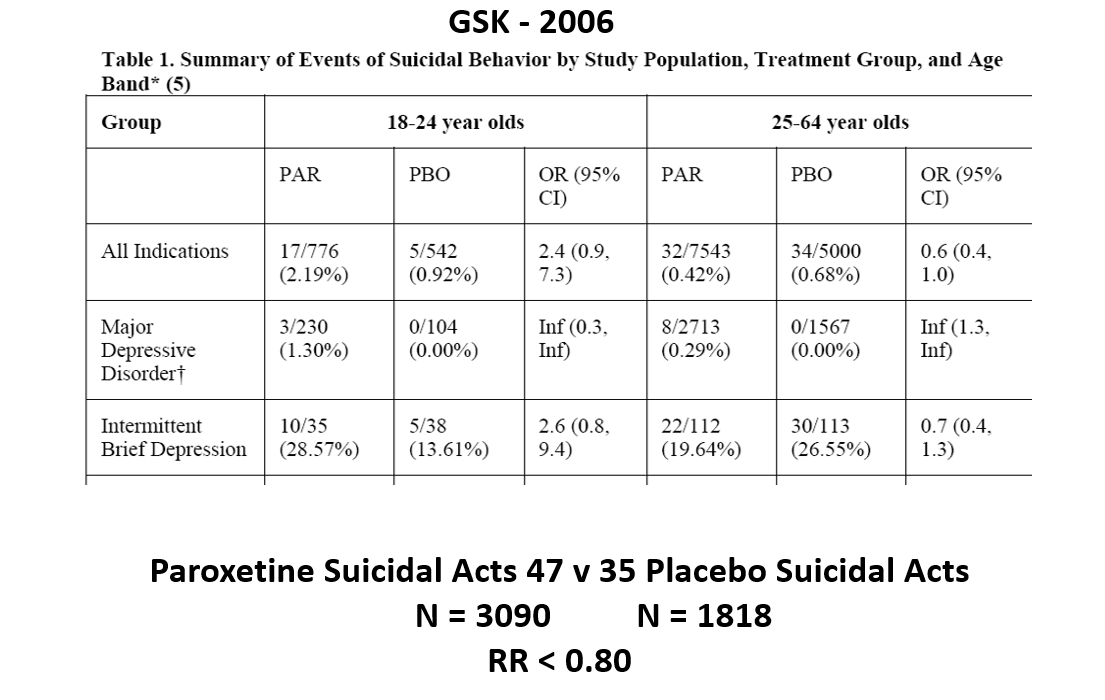
Slide 16: Other people say randomization controls unknown confounders. This slide shows some data straight from a 2006 GlaxoSmithKline paper. GSK’s SSRI paroxetine was in trouble – the RCTs data for Major Depressive Disorder seem to show paroxetine causes suicidal events. The real data I think are worse that GSK admit to here.
{kind=link}
Slide 17: But never fear RCTs come to the rescue. GSK also did trials in people with Intermittent Brief Depressive Disorders – IBDD. These are borderline personality disorder to most people – patients who have suicidal events much more often than anyone else. But these patients can meet criteria for depression and could be entered into Depression RCTs.
GSK did two trials of paroxetine in this group – the data didn’t look all that good. Here are IBDD data from the two GSK trials.
{kind=link}
Slide 18: When you add the IBDD data to the MDD data – all of a sudden paroxetine doesn’t cause suicidal events, it protects against them. We could add 12 more events to the paroxetine arm and still get the same magical outcome and 40 events before the company would have to concede their drug caused people to be suicidal.
Something like this is going to happen in every treatment trial where the patients entered are heterogenous – back pain, breast cancer, diabetes, hypertension, osteoporosis, parkinson’s disease. We can use an effect a drug causes to hide an effect a drug causes. RCTs are not a good way to work out what is going on.
{kind=link}
Slide 19: Let’s look deeper into RCTs. The first rating scale for behavior was the Hamilton Rating Scale for Depression. Here is Max Hamilton saying:
It may be that we are witnessing a change as revolutionary as was the introduction of standardization and mass production in manufacture. Both have their positive and negative sides
He saw the scale as a checklist of things to ask about in an interview – a mixed blessing.
{kind=link}
Slide 20: If you cleave to the checklist, you will do standardized but possibly disastrous interviews. For instance, on the scale, there is a suicide item. Suicidality can stem from the illness or the drug. This needs a judgement call – if caused by the drug you should rate the person as Zero – if caused by the illness you might rate 3 or 4. Ditto for sex, for sleep. If you just check yes for suicidality, the default is to the illness.
Checklists like these however are now viewed as scientific instruments. They look better to hospital..